Sgarbossa Criteria for Diagnosing Myocardial Infarction with LBBB
Sgarbossa Criteria are a set of rules doctors use to identify a heart attack in patients who have a Left Bundle Branch Block (LBBB) on their ECG. LBBB can make it hard to see typical heart attack signs, so these criteria help pick out the key changes. They guide timely diagnosis and treatment in emergency situations.
Sgarbosa Criteria calculator is intended for informational and educational purposes only. It should not be used as a substitute for professional medical advice, diagnosis, or treatment. Always consult your healthcare provider.
Electrocardiogram (ECG) Basics in MI
An electrocardiogram (ECG) captures the electrical activity of the heart to help in the diagnosis of myocardial infarction (MI). It views the heart from many different angles using a 12-lead system that includes limb and precordial leads. MI causes specific ECG abnormalities that relate to the impacted heart area, such as Q waves, T-wave inversions, and ST-segment elevation. As an example, an inferior MI is indicated by ST elevation in leads II, III, and aVF, whereas an anterior MI is indicated by elevation in V3-V4. Healthcare providers can determine the location and severity of a heart attack with the use of these patterns.
Overview of Left Bundle Branch Block (LBBB)
Left bundle branch block (LBBB) is a condition that occours when the electrical communication from the heart to the left ventricle is either stopped or delayed, causing an irregular movement of the left ventricle, causing irregular movements of the left ventricle. LBBB, which can often be found on an ECG without any symptoms, may be a sign of underlying cardiac conditions such valve disease, cardiomyopathy, hypertension, or coronary artery disease. Since LBBB typically doesn’t need direct care, treating the underlying issue is crucial. A cardiac resynchronization treatment (CRT) device may assist improve ventricular function in some types of heart failure.
Importance of Timely MI Diagnosis
A myocardial infarction (MI) must be diagnosed early in order to protect the heart muscle, prevent mortality, and help with healing. When the phrase “time is muscle” is meant that if the heart stays for a long time without oxygen the more damage is done. Early diagnosing and medical treatment, like clot-dissolving medications or angioplasty (PCI) to restore blood flow will greatly increase the survival rate and prevent hospitalization. To have the right timely diagnosing relies on the patients when seeking a rapid assistance, fast emergency response, and also using ECGs, blood test so the heart attack can be detected faster so the medical treatment cant be delayed.
Role of cardiac biomarkers in diagnosing MI with LBBB
Patients with a left bundle branch block (LBBB) the ECG might be complicated and could hide heart attack symptoms. Due to this, blood tests and heart damage, and especially troponin, have become very crucial. To make the right evaluation and confirming the heart attack, healthcare providers have a closer look for any rise or fall of troponin levels. BNP tests are mostly used for heart failure, but other tests, such as CK-MB, are less reliable. Healthcare providers in order to have the right diagnosing and evaluating it, they combine and see troponin results, symptoms and sometimes use the Sgarbossa criteria in order to have the right evaluation.
What is Sgarbossa Criteria?
Sgarbossa criteria is the collection of electrocardiogram (ECG) rules that are used to diagnose heart attacks in people with rapid heartbeats or Left Bundle Branch Block (LBBB), which makes it hard to detect a heart attack on a standard ECG. It helps healthcare providers in identifying specific changes in the ST segment that point to a persistent myocardial infarction. Modified Sgarbossa Criteria, is a newer version that has an improved accuracy by evaluating the ST-segment elevation to the heart’s typical electrical cycle rather than depending only on a fixed measurement. To say in simple words, the Sgarbossa criteria its an advanced ECG method that helps in detecting hidden heart attacks when the typical ECG symptoms are difficult to detect.
Components of Sgarbossa’s Criteria
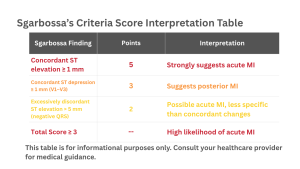
Concordant ST elevation: ST segment goes up in the same direction as the main QRS wave by ≥1 mm → likely heart attack.
Concordant ST depression: ST segment goes down by ≥1 mm in leads V1–V3 → may indicate a posterior heart attack.
Excessively discordant ST elevation: ST segment rises >5 mm in a lead where the QRS is mainly downward → possible heart attack.
Clinical Applications of Sgarbossa’s Criteria
Sgarbossa criteria is primarily used in helping doctors to immediately determine a heart attack in patients with a LBBB or rapid heartbeats, also is used in emergency and cardiology situations and when the ECG seems not normal and makes it complicated to diagnose. These criterias give the attention to specific ECG abnormalities that may still indicate a heart attack even when the typical symptoms are hidden.
In emergent situations they help doctors to make quicker decision on medical treatment, such sending the patients for an immediate (urgent) procedure to restore blood flow and avoiding possible dangerous delays. The sgarbossa criteria lbbb helps cardiologists in determining patients in high risk who could require immediate medical treatments. It is a helpful method that can help in making the right and precise diagnosing in situation where ECG interpretation is difficult.
Advantages of Sgarbssa’s Criteria
In clinical practice, the Sgarbossa Criteria offer a number of important advatanges. It improves the accuracy of the diagnosing, with the newer and improved modified version being much more sensitive while keeping good precision, and with a positive result suggesting a real heart attack. Doctors have the possibility to detect high risk patients faster, avoiding misdiagnosing , minimize the unecessary hard medical treatments with the support of immediate and time-sensitive decision-making of the criteria.
Sgarbosa Criteria is also helpful for patients with ventricular-paced rhythms problems, which assists in classifying risk by identifying patients with higher mortality risk. A positive Sgarbosa criteria test could lead the cardiac lab team to act right away to identify a blocked artery and restore blood flow.
Limitations of Sgarbossa’s Criteria
Beside being a useful method the sgarbossa criteria lbbb comes along with some limitations. The original version has a low specificity, that means in a negative result is not able to accurately identify a heart attack, and in patients with high QRS voltage may be confused by its fixed threshold for discordant ST-elevation.
The newer version has an increased sensitivity ,but on the other hand, it has slighty decreased specificity and need more complicated calculations, which can be more difficult to be implemented right in emergency situations. Both version rely on precise and accurate ECG interpretation, are aren’t meant to replace the medical clinical judgment, and might not be useful for paced rhythms or other atypical ECG patterns other than LBBB.
FAQs for Sgarbossa’s criteria
Can Sgarbossa criteria be applied to Right Bundle Branch Block (RBBB)?
No. Sgarbossa criteria were made for Left Bundle Branch Block (LBBB) and paced rhythms, which have a similar ECG pattern. Heart attacks in patients with RBBB need different rules to diagnose.
Are Sgarbossa’s criteria useful in patients with Left Ventricular Hypertrophy (LVH)?
Yes. The modified Sgarbosa criteria work even if a patient has LVH. LVH can make the heart’s ECG signals bigger, which could confuse the original rules. Using the ST/S ratio in the modified criteria helps avoid mistakes.
What does the clinical context add to the ECG interpretation?
The patient’s symptoms and condition are very important. A positive Sgarbossa score strongly suggests a heart attack, but a negative score doesn’t completely rule it out. Patients with ongoing chest pain or unstable vitals may still need urgent treatment. Repeating ECGs and checking troponin levels is essential.
Are there newer or alternative methods besides Sgarbossa’s criteria?
Yes. Newer methods, like the Barcelona algorithm, aim to improve accuracy. They refine the rules for ECG patterns. Despite these updates, Sgarbossa’s criteria are still widely used. Combining ECGs with high-sensitivity troponin tests gives an even clearer picture.
How should a clinician interpret a negative Sgarbossa result?
A negative Sgarbossa score does not guarantee there is no heart attack. If a patient shows MI symptoms (like chest pain), doctors should stay alert and use other tests, repeated ECGs, blood tests, or echocardiograms, to check for a heart attack.
Should patients with positive Sgarbossa criteria go to the cath lab?
Yes. A positive Sgarbossa result, especially using the modified criteria, is a strong sign of an acute heart attack. Patients with chest pain should be treated as having a STEMI and sent to a cardiac catheterization lab for immediate treatment.
Explore More Helpful Health Tools
We develop tools to help you take control of your well-being and make informed life choices. Explore our range of health resources, including our Sgarbossa Criteria Calculator , designed to support your mental and physical health.
Below you will find a couple of them and much more that are just a search away . If you don’t find any specific test or calculator you’re looking for please feel free to contact-us so we can create it for everyone.
Cardiac Output Calculator (Fick’s Formula)
Estimates the heart’s blood-pumping capacity using oxygen consumption and blood oxygen levels.
Glasgow-Blatchford Bleeding Score (GBS)
Assesses the risk of severe bleeding in patients with upper gastrointestinal bleeding.